
Abstract
The potential of “e-health” interventions in Anorexia Nervosa has been recognized over the past two decades, with a growing roster of apps, online resources and wearable technology. Recently, the adoption of glucose-sensing devices, developed for use in diabetes treatment, has opened the door for a plethora of new possibilities for Anorexia e-health delivery. This essay will outline how a novel feedback system, using glucose sensing coupled with artificial intelligence and integrated into a mobile app, could be the answer to effective and real-time implementation of dietary interventions in Anorexia Nervosa patients in a variety of settings.
Introduction
Anorexia Nervosa (AN) is a complex and debilitating eating disorder with some of the worst morbidity and mortality outcomes in psychiatry. AN can be particularly difficult to treat due to the powerful psychological maintaining factors centered around ideals of thinness, drive for lowering body weight and subsequent reactionary behaviors2,3. Typically, this may include aggressive restriction of calories, excessive exercise, purging or pharmaceutical abuse; with the outcome of rapid weight loss or low BMI4. Without effective management, AN has a tendency to a chronic, treatment refractory course5.
Due to factors which include stigma, perceived benefits of the disorder and skepticism of services, AN patients are less likely to engage with care than those with physical health conditions, or other psychiatric illnesses6. AN interventions typically centre around weight restoration through calorie-counting protocols and diet re-introduction7. Patients are required to adhere to mealtime schedules as inpatients or strict calorie targets in intensive day care or outpatient settings8,9. These interventions frequently fail to create lasting change, even with close supervision10. Calorie counting, along with choice of macronutrients is a labour-intensive process, especially for AN patients without supportive care givers11,12. Furthermore, covert purging behaviour, additional exercise and false calorie reporting is difficult to detect and can provoke confrontation between patient and care givers13,14.
Clinicians are turning to digital technology (“e-health”) for new ideas to improve patient experience and outcomes15,16,17. When used alongside traditional services, e-health shows promise and can be delivered via online courses, video-conferencing, text/email communication, mobile applications (‘apps’), virtual reality and increasingly, artificial intelligence (AI)18,19. If deployed correctly, e-health can reduce pressure on existing services and provide easy accumulation of data throughout a patient’s unique recovery journey.
Wearable technology as part of an e-health approach could prove to be a useful tool in AN treatment, providing opportunities for both patient and clinician. Germain et al have shown how continuous glucose monitoring devices (CGM) can be used to study the pattern of glycaemic regulation in anorexic patients, with no examples of patient noncompliance with the device20.
Building on Germain et al’s study, this essay explores coupling CGM, with artificial intelligence and a mobile app to provide a new tool to facilitate dietary reintroduction in AN. This technology could create real-time feedback on a patient’s eating patterns as well as correctly flagging instances of purging and fraudulent self-report.
Wearable CGM in AN
CGM has proved to be a successful feature of diabetes outpatient management21. Traditionally coupled to insulin delivery, the use of these devices for purely glucose sensing was employed by Germain et al in anorexic patients, after they identified the lack of diurnal measurement of glycemic status in AN research. Blood glucose (BM) measurement has been used up until this point only as a point-of-care test in severe AN physical decompensation22.
Their findings are striking. Not only did they identify that glucose levels are lower for longer periods of the day compared to previous data on healthy controls, they also suggest that CGM devices could be used to record actual calorific intake compared to self-reported intake. By plotting post-prandial glucose deltas and correlating them to calories consumed, this technology could flag up any false reporting of calorie intake and/or post-prandial purging.
Advances in CGM technology suggest that the devices will be well tolerated by AN patients. Apple Inc is poised to launch a new version of its Apple Watch, which will include a completely non-invasive CGM feature23. Such a device can be worn for months at a time with few if any risks of complications24.
Such a device could potentially create accountability for patients with respect to self-reporting of calories, an issue which has plagued dietary interventions throughout the history of AN, particularly in outpatient settings25.
Combining Glucose sensing with AI in a mobile app; A unified feedback system
Measuring glycaemic patterns in AN patients using CGM is an exciting strategy however, it is likely to fail without a complementary platform that can integrate BM data and calorie intake to give a digital readout of adherence to the relevant parties. Mobile apps could provide such a platform.
Apps are an example of a technology readily accessible to most ED patients and carers, and integration of mobile apps into the AN pathway is not a wholly new phenomenon26,27. However, it is of note that most studies focus on relapse prevention rather than the acute treatment phase28. Notwithstanding, user feedback on apps reinforces that they are highly acceptable to AN patients, and therefore represent an ideal hub for centralization of calorie and BM data; creating a de-facto feedback system (Figure 1)29.
The other role of the app is to serve as the interface for the recording of calorie intake. This can be best served through some recent advances in artificial intelligence technology. AI has been attempted already in ED with forays into chatbot programmes, with disappointing results30,31. However despite these setbacks, the use of AI does not have to be limited to these functions.
AI software from providers such as SnapCalorie, along with various copycats, is now capable of calorie counting meals based only from photographs of the plate of food32. Whilst still in its infancy, this AI calorie counting software has already been shown to give a reasonable fidelity in predicting calorie content for a variety of common meals and foodstuffs33.
This type of instant data may initially appear dangerous for AN patients with highly charged beliefs surrounding food, however in fact, conversion of calorie data from photographs may have the opposite effect and help to reduce the workload of calorie counting for both the patient and care-givers. Simple adjustments to this technology could allow patients and clinical teams with the option to hide or present quantitative data on calories according to individual patient preference and their stage of recovery. For example, presenting calorie content in discrete categories (“low, medium, high”) instead of continuous data could be beneficial to certain patients. Personalisation of the app toindividuals is also consistently listed as a desirable quality and could promote patient goal setting and adherence34,35. The quantitative data could then be made accessible to the clinician as needed.
Photography may further have the added benefit of giving the carers and clinical teams evidence of the type of foodstuffs AN patients are consuming, and identify early any detrimental patterns or facilitate dietician led adjustment to macro or micro nutrients.
Figure 1 provides a diagrammatical view of how these three techniques, BM sensing, mobile app and AI could combine to create a new digital feedback system. Clinical teams and patients agree to a dietary intervention, and patients will be able to passively evidence their adherence to the diet with photography and measurements of glycaemic patterns following calorie intake. Conversely, abnormal glycaemic measurements or absent photographic evidence would alert clinicians and caregivers to harmful purging or false self reporting of dietary intake, with the added advantage that regular BM sensing could also identify dangerous levels of hypoglycaemia and therefore those in need of medical stabilisation.
A system which is built on accountability between patient and clinician could drive better trust and limit the use of coercive and forced re-feeding practices.
Figure 1; Feedback system for AN dietary treatment
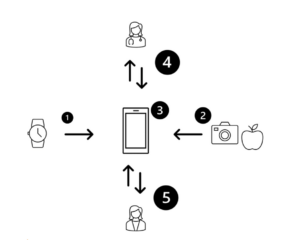
Data from wearable BM sensing devices (1) integrates with accurate calorie data generated by AI (2) to give an account of actual calorie intake vs. self-reported using an app (3). The app can communicate with clinicians and patients alike (4 & 5) to give real time feedback on adherence to dietary interventions
Limitations of the proposed technology
The feedback model proposed in Figure 1 is at this stage only a view of how to combine pre-existing techniques in new ways. It is important to note that the likely target population for this feedback system would be either inpatients under close supervision with 24 hour support or outpatients at an appropriate stage of recovery.
This is because AN cohorts frequently present challenges not seen in other study groups36,37. AN patients typically have higher rates of noncompliance, drop out and fraudulent self-report than almost any other psychiatric disorder38,39,40,41. The psychological drivers of the condition are often so strong that wearable technology, when combined with real time tracking, could even exacerbate the condition42. Furthermore, the presentation of any data collected must be handled sensitively to avoid similarly exacerbating pre-existing beliefs or creating power imbalance in the therapeutic relationship.
Despite these limitations, we should consider the likelihood that when coupling CGM with smart apps it will be much more difficult for AN patients to enact compensatory behaviours, driving open dialogue with their clinicians; drop outs will be easily identifiable. Close contact with a member of the parent team through the app could also be employed to readily identify patients who are struggling with the technology, in a similar manner to other mental health apps43.
More generally, the author recognises that apps are not immune from all manner of retention issues common to many e-health modalities, such as user dissatisfaction, lack of personalization, bug and glitching issues, technological illiteracy and lack of human connection44.
Despite this, we can take encouragement from user led feedback of previous e-health interventions that the use of apps is highly acceptable to most ED patients45. Furthermore, apps lend themselves well to other recordable features of qualitative experience, so additional arms could be added to the app which allow patients to self-journal their own experiences of the feedback system, along with positive affirmation either from the app or parent team following successful adherence to the dietary regimen.
Future directions
Following the recent Apple Inc announcement of the use of BM sensing technology into their new Apple wristwatch, it seems inevitable that diurnal and nocturnal variation in glucose will become yet another health metric to capture the public conscience46. No doubt this will similarly capture the attention of the ED world.
When it arrives, this should propel a new series of research into the use of glucose control at all stages of AN screening, treatment and recovery. Furthermore, the eating disorders field must be ready for another potential point of focus for vulnerable teenagers and adults and have experience with the technology well in advance before these patients appear in clinics and outpatient services fixated on glycaemic control. Why not embrace these metrics for treatment and be proactive with our approach to increasingly heterogenous health technology?
Conclusion
This essay has presented a potential new model for delivering dietary interventions in AN. The case has been made to combine AI based nutrition calculations, with wearable CGM technology to ensure patient adherence to dietary protocols and detect the use of purging behaviours early in the treatment phase. Pooling this data into an app will allow multidisciplinary team tracking of calorie intake andeasy recording of macro and micro nutrient profiles, as well as providing real time feedback on adherence.
In this way, it is hoped that mutual treatment goals and trust can be generated between the clinician and patient, leading to better shared decision making and continuity of care in inpatient and outpatient settings.
1 Eyza Koreshe et al., “Prevention and early intervention in eating disorders: findings from a rapid review,” Journal of Eating Disorders 11, no. 1 (March 10, 2023). https://doi.org/10.1186/s40337-023-00758-3.
2 World Health Organization (WHO) International Classification of Diseases, Eleventh Revision (ICD-11), 2019/2021
3 American Psychiatric Association. 2013. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association.
4 Hay, Phillipa J., Rebekah Rankin, Lucie Ramjan, and Janet Conti. “Current approaches in the recognition and management of eating disorders.” Medical Journal of Australia, June 25, 2023. https://doi.org/10.5694/mja2.52008.
5 Hay et al., “Current approaches in the recognition and management of eating disorders,” XXXX.
6 Kathina Ali et al., “What prevents young adults from seeking help? Barriers toward help‐seeking for eating disorder symptomatology,” International Journal of Eating Disorders 53, no. 6 (April 2, 2020). https://doi.org/10.1002/eat.23266.
7 Annette Cockfield and Ursula Philpot, “Managing anorexia from a dietitian’s perspective,” Proceedings of the Nutrition Society 68, no. 3 (May 6, 2009). https://doi.org/10.1017/s0029665109001281.
8 Andrea K. Garber et al., “A systematic review of approaches to refeeding in patients with anorexia nervosa,” International Journal of Eating Disorders 49, no. 3 (December 12, 2015). https://doi.org/10.1002/eat.22482.
9 NHS England. Adult Eating Disorders: Community, Inpatient and Intensive Day Patient Care Guidance for commissioners and providers, 000957 (London: National Collaborating Centre for Mental Health, 2019). https://www.england.nhs.uk/wp-content/uploads/2019/08/aed-guidance.pdf.
10 Enrica Marzola et al., “Nutritional rehabilitation in anorexia nervosa: review of the literature and implications for treatment,” BMC Psychiatry 13, no. 1 (November 7, 2013). https://doi.org/10.1186/1471-244x-13-290.
11 Cockfield and Philpot, “Managing anorexia from a dietitian’s perspective,”
12 Marzola et al., “Nutritional rehabilitation in anorexia nervosa: review of the literature and implications for treatment,”
13 Marzola et al., “Nutritional rehabilitation in anorexia nervosa: review of the literature and implications for treatment,” 14 Lucie Michelle Ramjan, “Nurses and the ‘therapeutic relationship’: caring for adolescents with anorexia nervosa,” Journal of Advanced Nursing 45, no. 5 (March 2004). https://doi.org/10.1046/j.1365-2648.2003.02932.x.
15 Shiri Sadeh-Sharvit, “Use of Technology in the Assessment and Treatment of Eating Disorders in Youth,” Child and Adolescent Psychiatric Clinics of North America 28, no. 4 (October 2019). https://doi.org/10.1016/j.chc.2019.05.011.
16 Rachel Dufour et al., “The use of technology in the treatment of youth with eating disorders: A scoping review,” Journal of Eating Disorders 10, no. 1 (November 24, 2022). https://doi.org/10.1186/s40337-022-00697-5.
17 Annika Wiebe et al., “Virtual reality in the diagnostic and therapy for mental disorders: A systematic review,” Clinical Psychology Review, October 2022. https://doi.org/10.1016/j.cpr.2022.102213.
18 Sadeh-Sharvit, “Use of Technology in the Assessment and Treatment of Eating Disorders in Youth,”.
19 José Alberto Benítez-Andrades et al., “Empowering machine learning models with contextual knowledge for enhancing the detection of eating disorders in social media posts,” Semantic Web, March 13, 2023. https://doi.org/10.3233/sw-223269.
20 Natacha Germain et al., “Continuous glucose monitoring assessment in patients suffering from anorexia nervosa reveals chronic prolonged mild hypoglycemia all over the nycthemeron,” European Eating Disorders Review, December 21, 2022. https://doi.org/10.1002/erv.2963.
21 P. J. Taylor et al., “Tolerability and acceptability of real-time continuous glucose monitoring and its impact on diabetes management behaviours in individuals with Type 2 Diabetes – A pilot study,” Diabetes Research and Clinical Practice 155 (September 2019). https://doi.org/10.1016/j.diabres.2019.107814.
22 Medical Emergencies in Eating Disorders: Guidance on Recognition and Management, CR233 (London: Academy of Medical Royal Colleges, 2023)
23 Mark Gurman, “Apple Makes Major Progress on No-Prick Blood Glucose Tracking for Its Watch,” Bloomberg, February 22, 2023, https://www.bloomberg.com/news/articles/2023-02-22/apple-watch-blood-glucose-monitor-could-revolutionize-diabetes-care-aapl?leadSource=uverify%20wall
24 Taylor et al., “Tolerability and acceptability of real-time continuous glucose monitoring and its impact on diabetes management behaviours in individuals with Type 2 Diabetes – A pilot study,”
25 Marzola et al., “Nutritional rehabilitation in anorexia nervosa: review of the literature and implications for treatment,”
26 Anneliese Haas et al., “Adapting a mobile app to support patients with anorexia nervosa following post-acute care: perspectives from eating disorder treatment center stakeholders,” Frontiers in Digital Health 5 (May 19, 2023): https://doi.org/10.3389/fdgth.2023.1099718.
27 Eyza Koreshe et al., “Prevention and early intervention in eating disorders: findings from a rapid review,” Journal of Eating Disorders 11, no. 1 (March 10, 2023). https://doi.org/10.1186/s40337-023-00758-3.
28 Christina Neumayr et al., “Improving aftercare with technology for anorexia nervosa after intensive inpatient treatment: A pilot randomized controlled trial with a therapist‐guided smartphone app,” International Journal of Eating Disorders 52, no. 10 (August 20, 2019). https://doi.org/10.1002/eat.23152.
29 Haas et al., “Adapting a mobile app to support patients with anorexia nervosa following post-acute care: perspectives from eating disorder treatment center stakeholders,”
30 Lauren McCarthy, “A Wellness Chatbot Is Offline After Its ‘Harmful’ Focus on Weight Loss,” New York Times, June 10, 2023, https://www.nytimes.com/2023/06/08/us/ai-chatbot-tessa-eating-disorders-association.html.
31 Gemma Sharp, John Torous, and Madeline L. West, “Ethical Challenges in AI Approaches to Eating Disorders,” Journal of Medical Internet Research 25 (August 14, 2023). e50696, https://doi.org/10.2196/50696.
32 Kyle Wiggers, “SnapCalorie taps AI to estimate the caloric content of food from photos | TechCrunch,” TechCrunch, June 26, 2023, https://techcrunch.com/2023/06/26/snapcalorie-computer-vision-health-app-raises-3m/?guccounter=1&guce_referrer=aHR0cHM6Ly93d3cuZ29vZ2xlLmNvbS8&guce_referrer_sig=AQAAAF1qjB79940zWqRzDtp-Vywm9GHSkoTYp8ukmT-7TFMjOiRRk7ZvEW-n6SWaNOMbwfBFd5lIGQ5aIJjsK4T1S0f6GjtVwUBCPMGSyA6evzGmhterLM74DfS9Uex0oA5kUZXWA0CKy705xChM5bwmQ1Kk8rTjnDmyk8QjKBXP6GyC.
33 Stephanie Van Asbroeck and Christophe Matthys, “Use of Different Food Image Recognition Platforms in Dietary Assessment: Comparison Study,” JMIR Formative Research 4, no. 12 (December 7, 2020). e15602, https://doi.org/10.2196/15602.
34 Dufour et al., “The use of technology in the treatment of youth with eating disorders: A scoping review,” 35 Koreshe et al., “Prevention and early intervention in eating disorders: findings from a rapid review,”
36 Catherine Boyd, Suzanne Abraham, and Georgina Luscombe, “Exercise behaviours and feelings in eating disorder and non-eating disorder groups,” European Eating Disorders Review 15, no. 2 (2007). https://doi.org/10.1002/erv.769.
37 Hay et al., “Current approaches in the recognition and management of eating disorders,”
38 Hay et al., “Current approaches in the recognition and management of eating disorders,”
39 Cecilia Vinchenzo, Catherine McCombie, and Vanessa Lawrence, “The experience of patient dropout from eating disorders treatment: a systematic review and qualitative synthesis,” BJPsych Open 7, S1 (June 2021). https://doi.org/10.1192/bjo.2021.792.
40 Hannah DeJong, Hannah Broadbent, and Ulrike Schmidt, “A systematic review of dropout from treatment in outpatients with anorexia nervosa,” International Journal of Eating Disorders 45, no. 5 (August 30, 2011). https://doi.org/10.1002/eat.20956.
41 Koreshe et al., “Prevention and early intervention in eating disorders: findings from a rapid review,”
42 Courtney C. Simpson and Suzanne E. Mazzeo, “Calorie counting and fitness tracking technology: Associations with eating disorder symptomatology,” Eating Behaviors 26 (August 2017). https://doi.org/10.1016/j.eatbeh.2017.02.002.43 Sarah Chang, Noy Alon, and John Torous, “An exploratory analysis of the effect size of the mobile mental health Application, mindLAMP,” DIGITAL HEALTH 9 (January 2023)., https://doi.org/10.1177/20552076231187244.
44 Haas et al., “Adapting a mobile app to support patients with anorexia nervosa following post-acute care: perspectives from eating disorder treatment center stakeholders,”
45 Haas et al., “Adapting a mobile app to support patients with anorexia nervosa following post-acute care: perspectives from eating disorder treatment center stakeholders,”
46 Mark Gurman, “Apple Makes Major Progress on No-Prick Blood Glucose Tracking for Its Watch,” Bloomberg, February 22, 2023, https://www.bloomberg.com/news/articles/2023-02-22/apple-watch-blood-glucose-monitor-could-revolutionize-diabetes-care-aapl?leadSource=uverify%20wall
Un uso novedoso de la tecnología wearable/portátil y la inteligencia artificial para avanzar en el tratamiento de la anorexia nervosa.
Abstract
El potencial de las intervenciones de “e-Salud”(también cibersalud, salud digital) en la anorexia nervosa se ha reconocido en las últimas dos décadas, con una lista cada vez mayor de aplicaciones, recursos en línea y tecnología portátil (también tecnología usable o salud móvil) Recientemente, la adopción de dispositivos de detección de glucosa, desarrollados para su uso en el tratamiento de la diabetes, ha abierto la puerta a una gran cantidad de nuevas posibilidades para la prestación de servicios de e-salud para la anorexia. Este ensayo describirá cómo un novedoso sistema de retroalimentación, que utiliza sensores de glucosa combinados con inteligencia artificial e integrado en una aplicación móvil, podría ser la respuesta para la implementación eficaz y en tiempo real de intervenciones dietéticas en pacientes con anorexia nervosa en diversos entornos.
Introducción
La anorexia nervosa (AN) es un trastorno de la conducta alimentaria complejo y debilitante con algunos de los peores resultados de morbilidad y mortalidad en psiquiatría1. La anorexia nervosa (AN) puede ser particularmente difícil de tratar debido a factores psicológicos poderosos de mantenimiento, centrados en los ideales de delgadez internalizados, el impulso por la reducción del peso corporal y las conductas reactivas o compensatorias subsiguientes2,3. Por lo general, esto puede incluir restricción calórica agresiva, ejercicio excesivo, conductas purgativas o uso indebido de fármacos, con el resultado de una pérdida de peso rápida o un IMC bajo¹4. Sin un manejo eficaz, la anorexia nervosa tiende a seguir un curso crónico y refractario al tratamiento5.
Debido a factores que incluyen el estigma, los beneficios percibidos del trastorno y el escepticismo hacia los servicios de atención, las personas con anorexia nervosa son menos propensas a vincularse con el tratamiento que aquellas con afecciones de salud física u otros trastornos psiquiátricos6. Las intervenciones AN suelen centrarse en la recuperación de peso mediante protocolos de recuento de calorías y la reintroducción de la dieta7. Los pacientes deben cumplir los horarios de las comidas cuando están ingresados o los estrictos objetivos calóricos en los centros de cuidados intensivos de día o en los ambulatorios8,9. Estas intervenciones a menudo no logran generar un cambio duradero, incluso con una supervisión estrecha10. El recuento de calorías, junto con la elección de macronutrientes, es un proceso laborioso, especialmente para los pacientes con AN que no cuentan con cuidadores que les presten apoyo11,12. Además, las conductas purgativas encubiertas, el ejercicio adicional y el reporte falso de calorías son difíciles de detectar y pueden provocar confrontaciones entre el paciente y los cuidadores13,14.
Los clínicos están recurriendo a la tecnología digital (“e-salud”) en busca de nuevas ideas para mejorar la experiencia y los resultados de los pacientes15,16,17. Cuando se utiliza junto con los servicios tradicionales, la e-salud es prometedora y puede prestarse a través de cursos en línea, videoconferencias, comunicaciones por texto o correo electrónico, aplicaciones móviles (“apps”), realidad virtual y, cada vez más, inteligencia artificial (IA)18,19. Si se implementa correctamente, la e-salud puede reducir la presión sobre los servicios existentes y facilitar la recopilación de datos a lo largo del proceso de recuperación específico de cada paciente.
La tecnología wearable/portátil, como parte de un enfoque de e-salud, podría resultar una herramienta útil en el tratamiento de la anorexia nervosa, brindando oportunidades tanto para el paciente como para los clínicos. Germain et al. han demostrado cómo se pueden utilizar los dispositivos de monitorización continua de glucosa (CGM, por sus siglas en inglés) para estudiar el patrón de regulación glucémica en pacientes con anorexia, sin que se hayan dado casos de incumplimiento del tratamiento por parte de los pacientes20.
Basándose en el estudio de Germain et al., este ensayo explora la combinación de CGM con inteligencia artificial y una aplicación móvil para proporcionar una nueva herramienta que facilite la reintroducción de alimentos en la anorexia nervosa. Esta tecnología podría generar retroalimentación en tiempo real sobre los patrones de alimentación del paciente, así como identificar correctamente episodios de conductas purgativas y de autoevaluaciones falsas.
CGM portátil en AN
El CGM ha demostrado ser una característica eficaz del tratamiento ambulatorio de la diabetes²¹. Tradicionalmente asociado al suministro de insulina, Germain et al. emplearon estos dispositivos para la detección exclusiva de glucosa en pacientes con anorexia, tras identificar la falta de mediciones diurnas del estado glucémico en la investigación sobre la anorexia nervosa. Hasta ahora, la medición de la glucosa en sangre (BM, por sus siglas en inglés) solo se ha utilizado como prueba en el lugar de atención en casos de descompensación física grave por anorexia nervosa²².
Sus hallazgos son sorprendentes. No solo identificaron que los niveles de glucosa son más bajos durante períodos más largos del día en comparación con los datos anteriores sobre controles sanos, sino que también sugieren que los dispositivos CGM podrían utilizarse para registrar la ingesta calórica real en comparación con la ingesta de autoevaluación. Al graficar las variaciones posprandiales de glucosa y correlacionarlas con las calorías consumidas, esta tecnología podría detectar reportes falsos de la ingesta calórica y/o conductas purgativas posteriores a las comidas.
Los avances en la tecnología CGM sugieren que los dispositivos serán bien tolerados por los pacientes con AN. Apple Inc. está a punto de lanzar una nueva versión de su Apple Watch que incluirá una función de monitorización continua de glucosa (CGM) totalmente no invasiva²³. Este dispositivo puede llevarse puesto durante meses sin apenas riesgo de complicaciones²⁴. Un dispositivo de este tipo podría fomentar la responsabilidad de los pacientes con respecto a la autoevaluación de calorías, un problema que ha afectado a las intervenciones dietéticas a lo largo de la historia de la AN, especialmente en entornos ambulatorios²⁵.
Combinación de la detección de glucosa con IA en una aplicación móvil; un sistema de retroalimentación unificado.
La medición de los patrones glucémicos en pacientes con anorexia nervosa mediante monitoreo continuo de glucosa (CGM) constituye una estrategia prometedora; sin embargo, es probable que resulte insuficiente sin una plataforma complementaria que integre los datos biomédicos y la ingesta calórica, a fin de proporcionar a las partes pertinentes una lectura digital del grado de adherencia. Las aplicaciones móviles podrían proporcionar dicha plataforma.
Las aplicaciones móviles son un ejemplo de tecnología fácilmente accesible para la mayoría de los pacientes con trastornos de la conducta alimentaria (TCA) y sus cuidadores, y la integración de apps móviles en los itinerarios de atención de la anorexia nervosa no es un fenómeno completamente nuevo²⁶,²⁷. Sin embargo, cabe destacar que la mayoría de los estudios se centran en la prevención de recaídas más que en la fase de tratamiento agudo²⁸. No obstante, la retroalimentación de los usuarios sobre las aplicaciones refuerza que estas son altamente aceptables para los pacientes con anorexia nervosa y, por lo tanto, representan un eje ideal para la centralización de los datos calóricos y biomédicos, creando un sistema de retroalimentación de facto. (Figura 1)²⁹.
La otra función de la aplicación es servir como interfaz para el registro de la ingesta calórica. Esto se puede lograr mejor gracias a algunos avances recientes en la tecnología de inteligencia artificial. La inteligencia artificial ya ha sido explorada en el ámbito de los trastornos de la conducta alimentaria, mediante incursiones en programas de chatbots, con resultados decepcionantes³⁰,³¹. Sin embargo, a pesar de estos contratiempos, el uso de la inteligencia artificial no tiene por qué limitarse a este tipo de funciones.
El software de inteligencia artificial de proveedores como SnapCalorie, junto con diversas plataformas similares, es actualmente capaz de estimar el contenido calórico de las comidas basándose únicamente en fotografías del plato de alimentos³². Aunque aún se encuentra en una fase incipiente, este software de conteo calórico basado en inteligencia artificial ya ha demostrado una fidelidad razonable en la estimación del contenido calórico de una variedad de comidas y alimentos de consumo común³³.
Este tipo de datos instantáneos puede parecer inicialmente peligroso para los pacientes con AN que tienen creencias muy arraigadas en torno a la alimentación; sin embargo, en realidad, la conversión de los datos calóricos a partir de fotografías puede tener el efecto contrario y ayudar a reducir la carga de trabajo que supone el recuento de calorías tanto para el paciente como para los cuidadores. Unos sencillos ajustes en esta tecnología podrían permitir a los pacientes y a los equipos clínicos ocultar o mostrar los datos cuantitativos sobre las calorías, según las preferencias individuales de cada paciente y su fase de recuperación. Por ejemplo, presentar el contenido calórico en categorías discretas (“bajo, medio, alto”) en lugar de datos continuos podría resultar beneficioso para ciertos pacientes. La personalización de la aplicación para cada individuo también se menciona constantemente como una cualidad deseable y podría promover el establecimiento de objetivos y el cumplimiento por parte de los pacientes³⁴,³⁵. Los datos cuantitativos podrían ponerse a disposición de los clínicos según sea necesario.
La fotografía puede tener además la ventaja añadida de proporcionar a los cuidadores y equipos clínicos pruebas del tipo de alimentos que consumen los pacientes con AN, e identificar de forma temprana cualquier patrón perjudicial o facilitar el ajuste de los macro y micronutrientes dirigido por un nutriólogo.
La Figura 1 presenta una representación diagramática de cómo estas tres técnicas —monitoreo biomédico (BM, por sus siglas en inglés), aplicación móvil e inteligencia artificial— podrían combinarse para crear un nuevo sistema digital de retroalimentación. Los equipos clínicos y los pacientes acuerdan una intervención dietética, y los pacientes podrán demostrar de forma pasiva su adherencia a la dieta mediante fotografías y mediciones de los patrones glucémicos tras la ingesta calórica. Por el contrario, las mediciones glucémicas anormales o la ausencia de evidencia fotográfica alertarían a los clínicos y a los cuidadores sobre conductas purgativas perjudiciales o autoevaluaciones falsas de la ingesta dietética, con la ventaja adicional de que el monitoreo biomédico regular también podría identificar niveles peligrosos de hipoglucemia y, por lo tanto, a quienes requieren estabilización médica.
Un sistema basado en la responsabilidad compartida entre el paciente y el clínico podría favorecer una mayor confianza y limitar el uso de prácticas coercitivas o de realimentación forzada.
Figura 1: Sistema de retroalimentación para el tratamiento dietético con AN.
Los datos provenientes de dispositivos portátiles de monitoreo biomédico (1) se integran con datos calóricos precisos generados por inteligencia artificial (2) para proporcionar un registro de la ingesta calórica real frente a la autorreportada mediante una aplicación (3) La aplicación puede comunicarse tanto con los clínicos como con los pacientes (4 y 5) para proporcionar retroalimentación en tiempo real sobre la adherencia a las intervenciones dietética.Limitaciones de la tecnología propuesta
El modelo de retroalimentación propuesto en la Figura 1 es, en esta etapa, solo una visión de cómo combinar técnicas preexistentes de nuevas maneras. Es importante señalar que la población objetivo probable para este sistema de retroalimentación serían los pacientes hospitalizados bajo estrecha supervisión con asistencia las 24 horas del día o los pacientes ambulatorios en una fase adecuada de recuperación.
Esto se debe a que las cohortes de anorexia nervosa presentan con frecuencia desafíos que no se observan en otros grupos de estudio36,37. Los pacientes con AN suelen presentar tasas más elevadas de falta de cumplimiento, abandono y autoevaluación fraudulenta que casi cualquier otro trastorno psiquiátrico38,39,40,41. Los factores psicológicos que provocan esta condición suelen ser tan fuertes que la tecnología portátil, cuando se combina con el seguimiento en tiempo real, podría incluso agravarla 42. Además, la presentación de cualquier dato recopilado debe tratarse con sensibilidad para evitar exacerbar creencias preexistentes o crear un desequilibrio de poder en la relación terapéutica.
A pesar de estas limitaciones, debemos considerar que, al combinar el CGM con aplicaciones inteligentes, será mucho más difícil para los pacientes con anorexia nervosa llevar a cabo conductas compensatorias, lo que podría favorecer un diálogo abierto con sus clínicos; además, los abandonos del tratamiento podrían identificarse con mayor facilidad. El contacto cercano con un miembro del equipo de padres a través de la aplicación también podría emplearse para identificar fácilmente a los pacientes que tienen dificultades con la tecnología, de manera similar a otras aplicaciones de salud mental43.
De manera más general, el autor reconoce que las aplicaciones no son inmunes a diversos problemas de retención comunes a muchas modalidades de e-salud, como la insatisfacción del usuario, la falta de personalización, errores y fallas técnicas, la baja alfabetización tecnológica y la falta de conexión humana44.
A pesar de ello, podemos sentirnos alentados por los comentarios de los usuarios sobre intervenciones de e-salud anteriores, que indican que el uso de aplicaciones es muy aceptable para la mayoría de los pacientes de TCA45. Además, las aplicaciones se prestan bien para registrar otros aspectos cualitativos de la experiencia, por lo que podrían incorporarse módulos adicionales que permitan a los pacientes llevar un autorregistro o diario de sus experiencias con el sistema de retroalimentación, junto con refuerzos positivos, ya sea generados por la propia aplicación o por el equipo de apoyo familiar, tras una adherencia exitosa al régimen dietético.
Direcciones futuras
Tras el reciente anuncio de Apple Inc. sobre la incorporación de tecnología de monitoreo biomédico en su nuevo reloj inteligente Apple Watch, parece inevitable que la variación diurna y nocturna de la glucosa se convierta en otra métrica de salud que capte la atención del público46. Sin duda, esto también llamará la atención del mundo de las TCA.
Cuando esto suceda, debería impulsar una nueva serie de investigaciones sobre el uso del control de la glucosa en todas las etapas de la detección, el tratamiento y la recuperación de la anorexia nervosa. Además, el campo de los trastornos de la conducta alimentaria debe estar preparado para otro posible punto de atención para adolescentes y adultos vulnerables y tener experiencia con la tecnología con suficiente antelación antes de que estos pacientes acudan a clínicas y servicios ambulatorios centrados en el control glucémico. ¿Por qué no aprovechar estas métricas para el tratamiento y adoptar un enfoque proactivo frente a una tecnología de salud cada vez más heterogénea?
Conclusión
Este ensayo ha presentado un nuevo modelo potencial para llevar a cabo intervenciones dietéticas en la AN. Se ha planteado la posibilidad de combinar cálculos nutricionales basados en inteligencia artificial con tecnología CGM portátil para garantizar que los pacientes cumplan los protocolos dietéticos y detectar el uso de comportamientos purgativos en una fase temprana del tratamiento. La recopilación de estos datos en una aplicación permitirá al equipo multdisciplinario realizar un seguimiento de la ingesta calórica y registrar fácilmente los perfiles de macro y micronutrientes, además de proporcionar información en tiempo real sobre el cumplimiento del tratamiento.
De esta manera, se espera que se puedan generar objetivos terapéuticos comunes y confianza entre los clínicos y los pacientes, lo que conducirá a una mejor toma de decisiones compartida y a la continuidad del tratamiento en entornos hospitalarios y ambulatorios.
1Eyza Koreshe et al., “Prevention and early intervention in eating disorders: findings from a rapid
review,” Journal of Eating Disorders 11, no. 1 (March 10, 2023). https://doi.org/10.1186/s40337-023-00758-3. 2 World Health Organization (WHO) International Classification of Diseases, Eleventh Revision (ICD-11), 2019/2021
3 American Psychiatric Association. 2013. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association.
4 Hay, Phillipa J., Rebekah Rankin, Lucie Ramjan, and Janet Conti. “Current approaches in the recognition and management of eating disorders.” Medical Journal of Australia, June 25,
2023. https://doi.org/10.5694/mja2.52008.
5 Hay et al., “Current approaches in the recognition and management of eating disorders,” XXXX.
6Kathina Ali et al., “What prevents young adults from seeking help? Barriers toward help‐seeking for eating
disorder symptomatology,” International Journal of Eating Disorders 53, no. 6 (April 2, 2020). https://doi.org/10.1002/eat.23266.
7 Annette Cockfield and Ursula Philpot, “Managing anorexia from a dietitian’s perspective,” Proceedings of the Nutrition Society 68, no. 3 (May 6, 2009). https://doi.org/10.1017/s0029665109001281.
8 Andrea K. Garber et al., “A systematic review of approaches to refeeding in patients with anorexia nervosa,” International Journal of Eating Disorders 49, no. 3 (December 12,
2015). https://doi.org/10.1002/eat.22482.
9NHS England. Adult Eating Disorders: Community, Inpatient and Intensive Day Patient Care Guidance for commissioners and providers, 000957 (London: National Collaborating Centre for Mental Health,
2019). https://www.england.nhs.uk/wp-content/uploads/2019/08/aed-guidance.pdf.
10 Enrica Marzola et al., “Nutritional rehabilitation in anorexia nervosa: review of the literature and implications for treatment,” BMC Psychiatry 13, no. 1 (November 7, 2013). https://doi.org/10.1186/1471- 244x-13-290.
11 Cockfield and Philpot, “Managing anorexia from a dietitian’s perspective,”
12 Marzola et al., “Nutritional rehabilitation in anorexia nervosa: review of the literature and implications for treatment,”
13 Marzola et al., “Nutritional rehabilitation in anorexia nervosa: review of the literature and implications for treatment,”
14 Lucie Michelle Ramjan, “Nurses and the ‘therapeutic relationship’: caring for adolescents with anorexia nervosa,” Journal of Advanced Nursing 45, no. 5 (March 2004). https://doi.org/10.1046/j.1365- 2648.2003.02932.x.
15 Shiri Sadeh-Sharvit, “Use of Technology in the Assessment and Treatment of Eating Disorders in Youth,” Child and Adolescent Psychiatric Clinics of North America 28, no. 4 (October
2019). https://doi.org/10.1016/j.chc.2019.05.011.
16 Rachel Dufour et al., “The use of technology in the treatment of youth with eating disorders: A scoping review,” Journal of Eating Disorders 10, no. 1 (November 24, 2022). https://doi.org/10.1186/s40337-022-
17 Annika Wiebe et al., “Virtual reality in the diagnostic and therapy for mental disorders: A systematic review,” Clinical Psychology Review, October 2022. https://doi.org/10.1016/j.cpr.2022.102213.
18 Sadeh-Sharvit, “Use of Technology in the Assessment and Treatment of Eating Disorders in Youth,”.
19 José Alberto Benítez-Andrades et al., “Empowering machine learning models with contextual knowledge for enhancing the detection of eating disorders in social media posts,” Semantic Web, March 13,
2023. https://doi.org/10.3233/sw-223269.
20 Natacha Germain et al., “Continuous glucose monitoring assessment in patients suffering from anorexia nervosa reveals chronic prolonged mild hypoglycemia all over the nycthemeron,” European Eating Disorders Review, December 21, 2022. https://doi.org/10.1002/erv.2963.
21 P. J. Taylor et al., “Tolerability and acceptability of real-time continuous glucose monitoring and its impact on diabetes management behaviours in individuals with Type 2 Diabetes – A pilot study,” Diabetes Research and Clinical Practice 155 (September 2019). https://doi.org/10.1016/j.diabres.2019.107814.
22 Medical Emergencies in Eating Disorders: Guidance on Recognition and Management, CR233 (London: Academy of Medical Royal Colleges, 2023)
23 Mark Gurman, “Apple Makes Major Progress on No-Prick Blood Glucose Tracking for Its Watch,” Bloomberg, February 22, 2023, https://www.bloomberg.com/news/articles/2023-02-22/apple-watch-blood-glucose- monitor-could-revolutionize-diabetes-care-aapl?leadSource=uverify%20wall
24 Taylor et al., “Tolerability and acceptability of real-time continuous glucose monitoring and its impact on diabetes management behaviours in individuals with Type 2 Diabetes – A pilot study,”
25 Marzola et al., “Nutritional rehabilitation in anorexia nervosa: review of the literature and implications for treatment,”
26 Anneliese Haas et al., “Adapting a mobile app to support patients with anorexia nervosa following post- acute care: perspectives from eating disorder treatment center stakeholders,” Frontiers in Digital Health 5 (May 19, 2023): https://doi.org/10.3389/fdgth.2023.1099718.
27 Eyza Koreshe et al., “Prevention and early intervention in eating disorders: findings from a rapid
review,” Journal of Eating Disorders 11, no. 1 (March 10, 2023). https://doi.org/10.1186/s40337-023-00758-3. 28 Christina Neumayr et al., “Improving aftercare with technology for anorexia nervosa after intensive inpatient treatment: A pilot randomized controlled trial with a therapist‐guided smartphone app,” International Journal of Eating Disorders 52, no. 10 (August 20, 2019). https://doi.org/10.1002/eat.23152.
29 Haas et al., “Adapting a mobile app to support patients with anorexia nervosa following post-acute care: perspectives from eating disorder treatment center stakeholders,”
30 Lauren McCarthy, “A Wellness Chatbot Is Offline After Its ‘Harmful’ Focus on Weight Loss,” New York Times, June 10, 2023, https://www.nytimes.com/2023/06/08/us/ai-chatbot-tessa-eating-disorders-association.html. 31 Gemma Sharp, John Torous, and Madeline L. West, “Ethical Challenges in AI Approaches to Eating Disorders,” Journal of Medical Internet Research 25 (August 14, 2023). e50696, https://doi.org/10.2196/50696. 32 Kyle Wiggers, “SnapCalorie taps AI to estimate the caloric content of food from photos | TechCrunch,” TechCrunch, June 26, 2023, https://techcrunch.com/2023/06/26/snapcalorie-computer-vision-health-app- raises- 3m/?guccounter=1&guce_referrer=aHR0cHM6Ly93d3cuZ29vZ2xlLmNvbS8&guce_referrer_sig=AQA AAF1qjB79940zWqRzDtp-Vywm9GHSkoTYp8ukmT-7TFMjOiRRk7ZvEW- n6SWaNOMbwfBFd5lIGQ5aIJjsK4T1S0f6GjtVwUBCPMGSyA6evzGmhterLM74DfS9Uex0oA5kUZXWA0CKy705xC hM5bwmQ1Kk8rTjnDmyk8QjKBXP6GyC.
33 Stephanie Van Asbroeck and Christophe Matthys, “Use of Different Food Image Recognition Platforms in Dietary Assessment: Comparison Study,” JMIR Formative Research 4, no. 12 (December 7, 2020).
e15602, https://doi.org/10.2196/15602.
34 Dufour et al., “The use of technology in the treatment of youth with eating disorders: A scoping review,”
35 Koreshe et al., “Prevention and early intervention in eating disorders: findings from a rapid review,”
36 Catherine Boyd, Suzanne Abraham, and Georgina Luscombe, “Exercise behaviours and feelings in eating disorder and non-eating disorder groups,” European Eating Disorders Review 15, no. 2
(2007). https://doi.org/10.1002/erv.769.
37 Hay et al., “Current approaches in the recognition and management of eating disorders,”
38 Hay et al., “Current approaches in the recognition and management of eating disorders,”
39 Cecilia Vinchenzo, Catherine McCombie, and Vanessa Lawrence, “The experience of patient dropout from eating disorders treatment: a systematic review and qualitative synthesis,” BJPsych Open 7, S1 (June
2021). https://doi.org/10.1192/bjo.2021.792.
40 Hannah DeJong, Hannah Broadbent, and Ulrike Schmidt, “A systematic review of dropout from treatment in outpatients with anorexia nervosa,” International Journal of Eating Disorders 45, no. 5 (August 30,
2011). https://doi.org/10.1002/eat.20956.
41 Koreshe et al., “Prevention and early intervention in eating disorders: findings from a rapid review,”
42 Courtney C. Simpson and Suzanne E. Mazzeo, “Calorie counting and fitness tracking technology: Associations with eating disorder symptomatology,” Eating Behaviors 26 (August
2017). https://doi.org/10.1016/j.eatbeh.2017.02.002.
43 Sarah Chang, Noy Alon, and John Torous, “An exploratory analysis of the effect size of the mobile mental health Application, mindLAMP,” DIGITAL HEALTH 9 (January
2023)., https://doi.org/10.1177/20552076231187244.
44 Haas et al., “Adapting a mobile app to support patients with anorexia nervosa following post-acute care: perspectives from eating disorder treatment center stakeholders,”
45 Haas et al., “Adapting a mobile app to support patients with anorexia nervosa following post-acute care: perspectives from eating disorder treatment center stakeholders,”
46 Mark Gurman, “Apple Makes Major Progress on No-Prick Blood Glucose Tracking for Its Watch,” Bloomberg, February 22, 2023, https://www.bloomberg.com/news/articles/2023-02-22/apple-watch-blood-glucose- monitor-could-revolutionize-diabetes-care-aapl?leadSource=uverify%20wall
